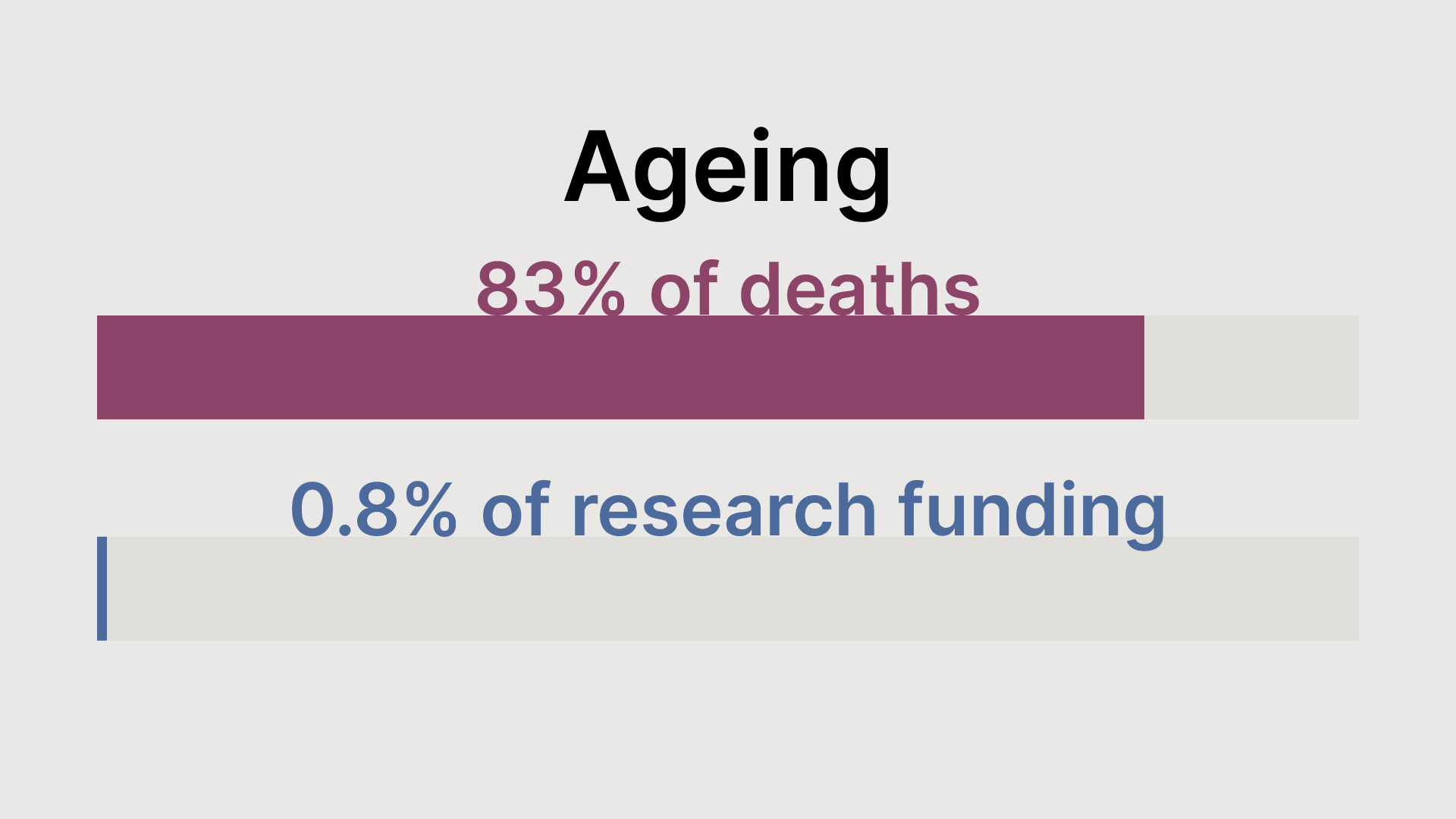
Ageing kills 83% of Americans. It gets 0.8% of the research budget.
Benjamin Franklin famously said ‘An ounce of prevention is worth a pound of cure’. At The Longevity Initiative, we believe that medicines that tackle ageing could be the ultimate form of prevention, reducing our risk of diseases from cancer to dementia all at once.
We would therefore hope that development of real anti-ageing treatments would be a research funding priority. Unfortunately, as the US-based Alliance for Longevity Initiatives (A4LI) highlighted in their new policy report, this is not the case in the United States.
In fact, of the $45 billion the National Institutes of Health (NIH) invested in biomedical science in 2024, just 0.8% went to ageing biology. For comparison, cancer research received around $8 billion, or roughly 18% of the total budget – in spite of cancer (and many other diseases) being primarily driven by the biology of ageing.
What kind of research does America fund?
One way to assess allocation of NIH funding is to compare investment in dollars per disease to the number of deaths it causes. Plotting this on a graph shows the striking disparity between diseases and dollars:

If funding were allocated in proportion to the number of deaths, the points would lie on a roughly straight line sloping from bottom left to top right – but they don’t. In fact, there’s almost no correlation, meaning that the amount of research funding a disease receives is essentially unrelated to how many Americans die from it.
Diseases that are high above the diagonal get relatively more funding per death, while those below get proportionally less. For example, cancer receives just over $8 billion of NIH research funding (primarily through the dedicated National Cancer Institute), and is listed on the death certificates of 720,000 Americans per year. Let’s call this a funding-per-death index of 1, and see how other conditions compare:

Cancer receives more funding per death than many other age-related causes. The largest mismatch is clear from the original scatter plot: heart disease appears on almost twice as many Americans’ death certificates annually, and yet receives just 22% of cancer’s funding. And conditions from sepsis to Parkinson’s disease receive far less funding per death than cancer.
Diseases which get most research funding per death
There are notable exceptions: on the graph, the two columns taller than cancer are research into coronaviruses, and Alzheimer’s disease. This means that they both receive more funding per death than cancer does – and they illustrate interesting reasons why funding for conditions should sometimes differ from the number of deaths caused by a given condition.
The reason for coronavirus research is obvious – there’s a long tail of covid-related research still ongoing after the global pandemic. One justification for this might be that, while the number of Covid-related deaths is mercifully far lower than at the pandemic’s peak in 2020–2021, coronaviruses are among the leading candidates for a future pandemic: perhaps channelling funds into coronavirus research will avert deaths from a hypothetical COVID-29 or COVID-37, which means the science deserves investment today.
It’s also not necessarily irrational for Alzheimer’s to receive more funding per death than cancer. It’s far more common to die with dementia than of dementia, but people spend years or decades gradually losing their memories, personalities and independence as they succumb to the disease. This means that they often need expensive long-term care, before actually dying of something else. Alzheimer’s is therefore a huge source of human suffering for patients and their loved ones and a substantial economic burden. Developing treatments for Alzheimer’s would avert a quantity of suffering higher than the corresponding death count might suggest, and save the US economy hundreds of billions a year.
Ageing fares worst
This brings us to the lowest funding index on the chart – indeed, the lowest figure across all the categories used in the dataset from which we drew these numbers – ageing. Ageing’s funding index compared to cancer is just 0.012 – it receives just 1.2% of the funding per death that cancer research does.
Worse, this misallocation doesn’t have a reasonable potential explanation: ageing biology is underfunded almost however you cut it. Since it is the root cause of by far the majority of diseases like cancer, dementia and so on, ageing is also mostly responsible for the human and economic toll these diseases inflict – plus the frailty, cognitive decline and so on, with their human and economic costs. That means that, were we to replot these graphs looking instead at lost years of healthy life, economic cost, and so on, ageing would be the standout underfunded field there too.
Put simply, investing in ageing has the potential to reduce suffering, improve the economic cost and reduce the time people spend with the disability and frailty that ageing brings. A4LI is right to call for more funding of ageing research to bring it closer in line with other conditions.
No disease is well-funded
It’s worth emphasising that, while ageing research receives the lowest level of funding given its potential impact, none of these figures is large in absolute terms. Cancer is the best-funded condition here, receiving just over $8 billion per year in research funding. This might sound like a lot but, shared among 335 million Americans, it’s $24 per person per year. On a per capita basis, heart disease receives $5.28 and dementia $10.80 – tiny sums for diseases with a significant chance of taking our lives, or the lives of someone we love.
In these terms, the underfunding of longevity science is even more stark: while the vast majority of Americans are likely to die of ageing, understanding its biology receives just $1.04 per American per year.
Economist Andrew Scott calculated that delaying ageing by a single year – meaning that everyone lived a year longer, and that additional year was in good health – would be worth $38 trillion to the US alone. That’s over $100,000 per American, a benefit so huge that it’s surely worth a few dollars per year to try to unlock.
Funding research by disease burden
Funding diseases based on the count of deaths they cause is still imperfect, as we’ve seen – some diseases have a large human or economic cost beyond their death rate, or could cause deaths in future in spite of a low death count today.
An ideal framework would attempt to take this into account and might be based on some combination of: current and likely future deaths from a disease; its wider social and economic burden on society; the likely effectiveness of an additional dollar of research funding, and some measure of how likely the research might be to impact multiple diseases or conditions. It would also be worth factoring in international impact, eg, for diseases like malaria that claim many lives in poorer countries who can’t afford NIH-scale research programmes of their own.
This would be a tough equation to solve, and necessarily somewhat imperfect – but it could be a huge improvement on what we have today. As A4LI explains in their paper, the way we fund medical research is essentially a series of historical accidents: ‘The strongest predictor of current NIH funding is historical allocation from previous decades, not contemporary burden of disease.’
Cancer research saw a substantial spike in funding in 1971, when President Nixon famously declared the ‘War on Cancer’. No politician wants to be the one who cuts cancer research and so, broadly speaking, the level has stayed high relative to other conditions.
Perhaps it’s time for a realignment, and a declaration of war to avert human suffering through medical research.
You can read more in A4LI’s policy paper, which sets out how NIH could increase funding for the upstream biology of ageing through cross-institute partnerships. If you’d like to add your name to their campaign for better-funded ageing research, you can do so here.
Notes on the data
The US is unusual in that it has a national register of research funding by disease, called the Research, Condition, and Disease Categorization (RCDC) system. It uses an automated text-mining system to classify grants by the diseases and conditions they address. This is used to publish an official table of research funding by disease area, which we used to make the graphics in this post.
Importantly, neither the research classification nor the mortality data in this table are exclusive. For example, a grant on how high blood sugar can damage the kidney might be classified as both diabetes and kidney disease. The grant is counted in full for every category it’s eligible for, meaning that you can’t add the figures together – the total funding in this table exceeds the total NIH budget by a factor of about seven!
The same is true of the deaths data: someone who died of a heart attack but also had advanced cancer might have both listed on their death certificate, and that would be counted as a death for both conditions. This means the total deaths reported here aren’t meaningful either. This is in some sense fairer: just because a heart attack happened to be what took someone’s life, it doesn’t mean we should ignore their advanced cancer when considering the human impact of diseases.
However, regrettably, the value for ageing in the RCDC table includes lots of research that we at The Longevity Initiative wouldn’t call ageing science. It is overwhelmingly concentrated on dementias – and diseases that increase in prevalence with age. The figure we used is the $347 million budget of the division within the National Institute on Aging (the Division of Aging Biology), the sole part of NIH primarily engaged in what we would classify as longevity research.
RCDC also doesn’t include a value for the number of deaths due to ageing. We calculated these using excess mortality above a ‘young adult’ baseline, based on CDC WONDER data. (This is based on methodology originally developed by Andrew Steele for his book, Ageless.) This counts all deaths in over-40s that happen at above the death rate of 35–39-year-olds as caused by ageing, which captures all of the various ways in which risk of death increases.
You can view all of the calculations for this post in a Google Sheet here.